
The emotion of anger has two facets:
-
Protective Facet: This function of anger is designed to protect us from predators. The predator represents a tremendous threat to us requiring a very violent response. Anger is potentially a very violent and savage emotion – too violent for the family and social relationships. In family and social relationships we need to shift our expression of anger over into the social-communicative function of anger.
-
Social Facet: The social-communicative facet of anger is to signal hurt, and it seeks empathy for our hurt. Within the social-communicative function of anger, the underlying social function is to create empathy: “You hurt me so I hurt you. You now feel the hurt that I feel. You now understand the hurt that I feel.” – the social-communicative function of anger is to establish a primitive form of empathy.
When the social-communicative facet of anger is not properly understood, then the danger becomes our indulging of the hurtful emotional violence of the protective facet of anger. We attack the other person with our anger to hurt them, and they defend themselves with their anger against our hurting them with our anger. The anger and hurt escalate.
Expressing Anger
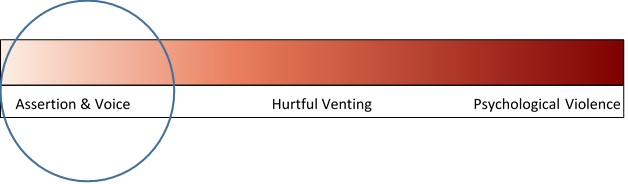
Expressing anger in a social context is seldom, if ever, productive. When we communicate our anger it should always remain a well-modulated expression of annoyance, assertive power, and authoritaive voice rather than the direct venting of anger.
On a 1-10 scale, the social expression of anger should never rise above a 3.
The emotion of anger is designed to defend against the predator. It is a savage and violent emotion. It is too violent for social communication and it savages relationships. But anger makes us feel powerful and brings with it the strength of absolute certainty. In the heat of anger we tell ourselves, “I don’t care” as we abandon ourselves to the powerful feelings of venting our anger. When we indulge our anger we savage relationships. Venting anger is self-indulgent.
In social communication and within the family, it is NEVER okay to indulge the expression of anger. Not in the marital relationship, not in the parent-child relationship. Anger within the family and social group is a communicative signal of underlying hurt indicating that an empathic breach has occurred in the relationship. In the family and social group, anger is a communicative social signal not an emotion that is to be indulged and vented.
In the family and social group, anger should remain a well-modulated expression of annoyance and concern (a 1 to 3 on a ten-point scale). It can carry the assertive strength and power of the underlying brain state, but we need to refrain from indulging the brutality of the emotion.
The venting of anger above a 4 on a ten-point scale represents an emotional assault delivered against the other person. It is just like hitting the other person with our fist, but instead of using our physical fist we are using an emotional fist. It is NOT okay to hit someone physically, it is not okay to hit someone emotionally. Indulging the venting of anger is not okay.
Anger management will be addressed in a separate essay, but it benefits greatly from both parties understanding the socially communicative (rather than the protective-aggressive) function of the emotion. Within its socially communicative function, anger indicates that a breach has occurred in the empathic field of shared understanding, and the anger represents a very primitive attempt to restore empathy (“You hurt me so I’ll hurt you, so that you’ll now understand the hurt that I’m feeling”).
Hurt (sadness) is a social emotion, whereas anger and fear are power emotions (dominance and submission respectively). The social function of hurt and sadness is to draw nurture when we communicate our hurt and sadness into the social field. In socially managing our anger, we want to recognize that the signal function of anger indicates that we feel hurt by something the other person said or did, and we then quickly transfer the communication away from anger and over into our hurt (sadness) which will draw nurture and restore the empathic relationship that was breached by the other person’s seemingly insensitive comment or action.
From a social communication standpoint, we want to translate our anger into hurt and communicate the hurt. Our communication partner also wants to recognize the social communicative function of anger as signaling a breach in empathic understanding, which will allow our communication partner to respond in the most productive fashion – reflective listening and understanding.
Restoring Empathy: “Tell me more about that.”- “Oh, so when I did X you felt Y?” – “I’m sorry. What can I do to make it up to you?”
All of this represents an intent to understand the other person from the other person’s point of view. An intent to understand restores empathy and decreases the other person’s anger.
We want to avoid the unproductive and escalating responses of defending, minimizing, and counterattacking.
Defensive Responding: “It’s not my fault” – “You’re overreacting.” “What about what you did? You did xyz and that hurt MY feelings.”
Since anger is an attack, our natural response is to defend. We defend ourselves by trying to convince the other person that we don’t deserve the criticism, that there were reasons for our actions or that the angry response of the other person is excessive and out of proportion, or we counter-attack to equalize the criticism.
All of these responses maintain the empathic breach which created the other person’s anger. In all of these responses we are asking the other person to understand us. Meanwhile, the other person’s anger is signaling that they are hurt because of our empathic failure with them, and they want us to understand their hurt, to nurture their hurt and make it better (to understand and apologize).
The Levels of Anger
The emotion of anger has three levels. The top two levels are:
“You hurt me so I hurt you” 
Anger is a defensive emotion. Anger arises when we are hurt (or are afraid we might be hurt), and anger is designed to prevent our being hurt by inflicting hurt on the threat.
The social function in communicating anger is to induce a submissive response in the other person that will generate an apology – the apology represents empathy for the hurt that was caused, which then created the angry-protective response.
Underneath the anger is hurt. In social-communicative anger there is an aggrieved party who is hurt – the person who is expressing the anger – and there is an offending party – the person who caused hurt and is therefore receiving the anger.
Aggrieved Party: The person who is expressing the anger. This person must quickly stop expressing anger and begin expressing the hurt.
Offending Party: This person had an “empathic failure” toward the aggrieved party that caused a hurt. Empathic failures are totally okay, common, and healthy social relationship sequences. They happen all the time. No big deal. When the other person goes “ouch” (becomes angry with us), we simply listen and understand our empathic failure, and we apologize to restore the empathic field. No big deal.
Beneath anger is hurt – “You hurt me – So I hurt you.”
So anytime we see anger we want to then look for – and respond to – the hurt that’s underneath.
The Core of Social Anger
The third level down is the most interesting – and the most productive. The reason you hurt me is because:
- “I care about you, and you don’t care about me.”
At its fundamental level, anger emerges from an empathic failure, and the anger represents a very primitive effort at restoring empathy:
- “I’ll hurt you so you’ll know how much you hurt me.”
That’s the structure of anger. You hurt me, so I hurt you. And the reason you hurt me is because I care about you but you don’t care about me.
Anger essentially arises from an empathic failure of the offending person for the feelings of the injured person. This empathic failure by the offending person breaches the bonded relationship with the injured person and creates the emotional injury. The injured person then responds with anger toward the offending person in retaliation for the hurt and in an effort to protect against being hurt by reestablishing the empathic bond – “You hurt me so I hurt you, and when you understand how much you hurt me you’ll stop… because you care about me and you don’t want to hurt me.”
When someone is angry with us, this is a social communication that we have done or said something that has hurt the other person’s feelings – we have had an empathic failure for the feelings and needs of the other person.
When we are angry at someone else, this is a communication from our emotional system that something the other person said or did hurt our feelings. They failed to be empathically attuned to what we were feeling and needing.
This is important to understand: Empathic failures that create relationship breaches and bursts of anger are TOTALLY NORMAL and entirely healthy relationship experiences. We cannot possibly remain empathically attuned to everyone all the time. We are separate individuals. Sometimes we say or do things that are not empathically attuned to the other person. This is okay.
The issue is not that we had an empathic failure toward this person. The issue is what do we do about it.
Inhibitory Networks
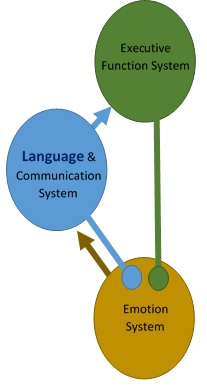
When we bring our emotions into the Language and Communication Systems, a set of inhibitory networks become active that go back to the Emotion System and quiet the intensity of the experienced emotion.
The goal of developmentally supportive parenting is to facilitate the child’s ability to bring emotional experience into language and communication, and to release and resolve the emotions through the healthy and bonded relationship with the parent.
When the child expresses anger, our initial response as parents is to seek to end the angry tantrum. We naturally view the child’s anger as a “problem behavior” to be suppressed.
However, when we simply try to suppress the child’s anger we are actually continuing the empathic breach that created the anger. Instead, a more productive response to the child’s anger is to “scaffold” the child’s ability to use emotions as a communicative signal. Rather than the explosive-expressive display of anger, we want the child to communicate. Children will not communicate if we don’t listen.
So our first response should be to listen – an intent to understand the child’s world from the child’s perspective. Something is hurting the child, that’s what is producing the anger. So what is hurting the child? This is the key question. Approach the child’s anger with this question in mind – what is hurting?
As we approach with this question, with this intent to understand the child’s world from the child’s perspective and to translate the child’s anger into hurt, we scaffold the development of the child’s brain networks for EXACTLY this same process of self-reflection, self-awareness, and understanding anger as an emotional signal of hurt.
And when we listen to the child’s anger AS IF the emotion has communicative value, then the child will make increasingly more sophisticated efforts to communicate with us. As the child brings his or her anger into the language and communication networks, the inhibitory networks of the Language and Communication System (and Executive Function System) activate to decrease the experience of anger, so that anger becomes annoyance. This is the goal of developmentally supportive parenting – to scaffold the development of these networks by “use-dependent” processes.
We build what we use.
Listening – Not Gratifying
We don’t necessarily have to gratify the child’s expressed needs by giving the child what the child wants. We are the parents, the adults, and the leadership function in the family is our responsibility. An important maturation domain for children is that they don’t always get what they want when they want it, and they must learn how to cope appropriately with the difficult emotions of frustration and disappointment.
However, even in teaching this important life lesson, we can at least be kind and empathetic to how difficult this life lesson is for the child – we can at least care about the child’s hurt and listen to the child. Perhaps there is some compromise that can be reached. Perhaps the child can have the desired object or activity at a future time, or perhaps the child can work to achieve the desired activity or object.
Are there times that we wanted something very much and have felt frustrated and disappointed that we couldn’t obtain the object of our desire? Of course. Are frustration and disappointment difficult and painful feelings? Yes, of course they are. So we can at least have empathy for how hard and painful it is for our children to learn these difficult life lessons and cope with the painful feelings of disappointment and frustration. We can listen to their pain, and provide nurture for their hurt, even as we set boundaries and limits on their desires and wants.
The child has a desire. We set a limit (we say, “No”). This creates the empathic failure on our part, we are failing to understand how much the child wants the object-of-desire. Our empathic failure in saying, “No” creates pain for the child which then becomes a display of anger.
In developmentally supportive parenting, instead of initially responding to the anger we instead respond to the child’s hurt and disappointment. In responding to the child’s hurt that is underneath the anger display, we are bringing to the child our intent to understand the child’s world from the child’s point of view, we are bringing empathy that restores the empathic bond and heals the cause of the anger. In this way we help the child communicate his or her hurt and disappointment rather than collapsing into an explosive-expressive display of anger.
Our goal is to bring the child’s expression of anger into the social field of appropriate social communication, and to help the child accurately recognize his or her hurt that is signaled by the anger.
Children will not communicate if we don’t listen.
Closure
Listening to the child does not necessarily mean giving the child what the child wants. We are the parents, the responsibility for leadership in the family is ours. The child must learn to adjust to and cope with limitations and restrictions in a socially appropriate way.
So after we respond with an appropriate period of listening and empathy – fostering the child’s communication – we can then bring the discussion to a close with an executive decision.
In some cases, when we listen to the child there may be some compromise we can reach. For example, instead of getting the child a candy snack at the store we may be able to work out a compromise through negotiation with the child to get the child a more appropriate and acceptable snack.
We build what we use.
Socially appropriate expression of desires, discussion, negotiation, and compromise are all positive pro-social communication skills.
In other cases, learning to cope appropriately with frustration and disappointment are also pro-social life skills.
Leadership within the family belongs to the parents. Closing discussion and making executive leadership decisions is the prerogative and responsibility of the parent.
What developmentally supportive parenting does is add a period of pro-social communication of emotion into the parent-child relationship in order to build in the child’s brain systems (through use-dependent processes) the interconnected networks between the Emotion System and the Language and Communication System.
The emotion of anger communicates hurt – due to an empathic failure. Developmentally supportive parenting responds to the hurt underneath the anger and in doing so fosters the child’s communication of this hurt and restores the empathic field that was breached and that caused the hurt.
Then – the parent moves on into closure of either compromise or an executive leadership decision.
Calm and Confident Authority
We don’t need to over-react to the child’s anger. The child is feeling overwhelmed by the pain of disappointment and frustration. Disorganized behavior is produced by a disorganized brain. A disorganized brain is painful.
We can help the child recover from this disorganized state by our remaining calm and confident in our authority and leadership as parents. The child is having a difficult time building the various brain networks needed to effectively regulate emotions. That’s okay, and that’s normal. The child’s anger simply represents a “protest behavior” produced by a disorganized brain state which is designed to elicit our involvement. The child is simply signaling a need for our supportive help. A developmentally supportive response will help the child build the needed underlying brain networks by scaffolding the use-dependent development of these brain networks.
The first and most primary connection is from emotions into and through the Language and Communication System. We scaffold the development of this connection by listening – by responding as if the child’s emotions have communicative value, which they do. Anger communicates hurt and an empathic breach in the relationship. Listen to the hurt, restore the empathic bond, and build this brain wiring between the Emotion System and the Language and Communication System.
Do this once, do this twice, do this 10,000 times, and the brain networks for the child’s pro-social communication of emotional experience rather than the explosive-expressive venting of emotions become stronger and more efficiently integrated. We build what we use.
Craig Childress, Psy.D.
Clinical Psychologist, PSY 18857
PS. All of these principles work equally as well in the marital relationship. What I do all the time in marital therapy is to first translate the spousal anger into hurt, and then into the more fundamental level of a desire for bonding (that’s being frustrated by an empathic failure of some kind).

 the scaffolding support is gradually withdrawn.
the scaffolding support is gradually withdrawn. the child in navigating these ever-evolving developmental challenges to build (through use-dependent processes; we build what we use) the integrated brain networks necessary for the child’s own successful self-responsibility and self-reliance.
the child in navigating these ever-evolving developmental challenges to build (through use-dependent processes; we build what we use) the integrated brain networks necessary for the child’s own successful self-responsibility and self-reliance.